Injuries involving the anterior cruciate ligament (ACL) of the knee are incredibly common these days. They are particularly prevalent amongst professional athletes and given the required time away from sport, they are certainly well covered in the media. Here are a few pointers surrounding injury mechanisms, assessment procedures and rehabilitation options if you have suffered a suspected ACL injury.
The problem
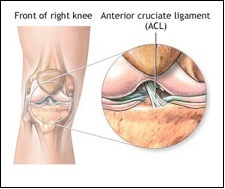
- The ACL is the stabilising ligament of the knee, and acts to prevent buckling of the knee
- The mechanism of injury is usually from a pivoting action on a grounded foot, usually during sport.
- Injury can be as a partial or total rupture and management may change according to degree of damage
- When the ACL is completely torn, surgery is a strong possibility to reconstruct the ligament
ACL ruptures usually occur with non-contact, pivoting injuries where the foot of the affected leg remains stuck to the ground. Typical examples include during a mistimed sidestep during a soccer match while wearing studded boots, or when falling during skiing at low speeds, when the ski bindings fail to release. Typically there is a cracking sound, immediate pain and swelling. The time it takes for pain to subside varies greatly between individuals. Many people who have suffered an ACL injury fail to recognise its significance initially because they are quickly able to walk, and even run is straight lines, without pain. They quickly find, however, that an unidentified ACL injury will give rise to sensations of instability or “giving way” during twisting or pivoting movements.
ACL Injury Symptoms
- Immediate swelling and bruising of the knee
- The knee will feel ‘unstable’ and may buckle or give way on you
- A ‘pop’ or ‘crack’ sound is often heard during injury
- Usually there is initial pain, although with a complete tear the pain subsides quickly (within minutes) but the knee often feels ‘unstable’, and may give way
- Often ACL injuries can occur in combination with injuries to other structures such as the medial collateral ligament or medial meniscus
ACL Injury Treatment
ACL injuries often occur in combination with damage to other structures, such as the medial meniscus or medial collateral ligament, so it is fair to say there is a big variation of presenting symptoms between one person to the next; from slight discomfort through to bellowing pain and disability.
If you have injured your knee and suspect an ACL tear, it is important to follow the RICE rules for acute injuries. They are: rest (avoid painful activities), ice (20 minutes every couple of hours is the current convention), compression (using a Tubigrip or compression bandage) and elevation (above the level of your heart if you can). Then get yourself in with your physio for a thorough assessment.
- Initial injury management is as for most soft-tissue injuries;
- Rest and immobilise, use crutches to assist with walking
- Ice for 20 minutes every 2-3 hours for the first 3 days
- Elevation, as able, lying on your back with leg elevated
- Seek diagnosis by seeing your GP or visiting one of the experts at Sydney Sports & Orthopaedic Physiotherapy, and the decision to confirm with imaging such as MRI may be made at that time
ACL Injury Management
Management for an ACL injury involves a visit to your physiotherapist who can test your knee for ligament deficiencies. If an ACL tear is suspected, you will usually be referred to an orthopaedic surgeon, who specialises in ACL reconstruction procedures, for further assessment and opinion. Sometimes the surgeon may ask for you to have an MRI scan, however, in some instances, the diagnosis can be obtained confidently with clinical testing.
Do you need Surgery for an ACL Injury?
- ACL tears require review by an Orthopaedic Surgeon
- The surgeon will discuss with you both conservative and surgical options
- A full tear may be managed with a surgical reconstruction, using a patellar tendon or hamstrings graft, or more recently with a synthetic ligament (LARS)
If an ACL rupture is confirmed, the surgeon will discuss your options with you. Some people are able to fulfil their desired activities without the need for surgery, however today’s conventional approach is to look toward reconstruction surgery if your lifestyle is likely to involve any twisting-type activities. These can include anything from playing backyard soccer with the kids to competing at the Rugby World Cup. Your physio will be around to ensure you regain all of the required strength and flexibility to return to the activities you love whether you decide to undergo surgery or not. The most common reconstruction procedures require up to 12 months before return to play is recommended.
More information
- A knee reconstruction will mean time away from sport and significant rehabilitation
- Return to sport in most cases is after 6 months
- Unloading the tendon in the initial phases will help with pain. These can include taping, heel raises and orthotics
At Sydney Physiotherapy Solutions our highly qualified physiotherapists specialise in the assessment, treatment and prevention of neuromusculoskeletal injuries.